- NEED HELP? CALL US NOW
- +919995411505
- [email protected]
WARTHIN’S TUMOR
Introduction
Warthin's tumor, also known as papillary cystadenoma lymphomatosum, is a benign cystic tumor of the salivary glands containing abundant lymphocytes and germinal centers (lymph node-like stroma).
OR
Warthin's tumor is an adenoma composed of bilayered columnar and basaloid oncocytic epithelium that forms multiple cysts with numerous papillae, accompanied by a proliferation of follicle-containing lymphoid tissue
It is named for pathologist Aldred Scott Warthin, who described two cases in 1929
Warthin’s tumor is second most common benign salivary gland tumor
Epidemiology
- Warthin tumor is the most common ‘monomorphic’ adenoma of the major salivary glands.
- It accounts for about 2% to 15% of all parotid tumors
- M>F
- Most common site Tail of parotid
Causes
- The exact underlying cause of Warthin tumor is currently unknown.
- However, smoking is thought to increase the risk of developing the tumor.
- Some studies suggest that radiation exposure and autoimmune disorders may also be associated with Warthin tumor
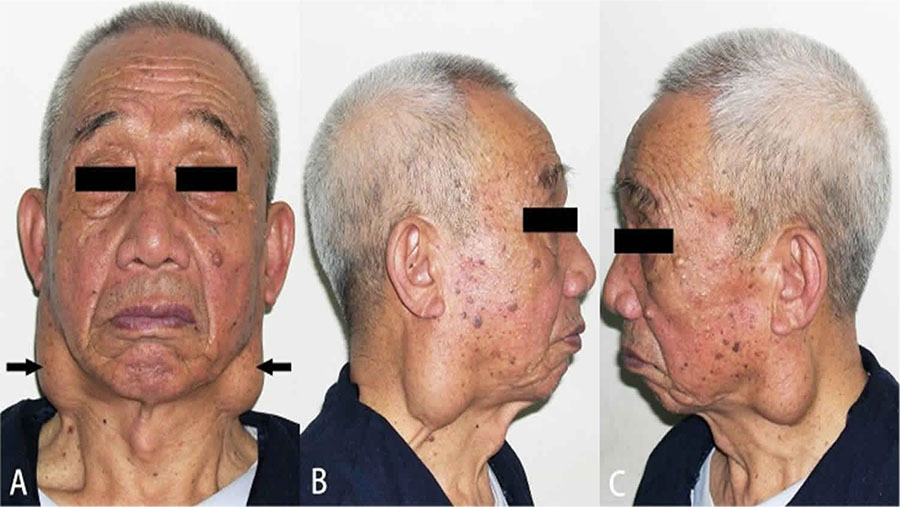
Signs and Symptoms
- Firm, usually painless swelling in one of the salivary glands (in front of the ears, under the chin, or on the floor of the mouth).
- Swelling can progress at varying rates depending on the underlying cause.
- Slow swelling usually indicates a benign tumor, while rapid swelling is more likely to indicate a malignant tumor or infection.
- Difficulty moving one side of the face, known as facial nerve palsy.
- This can signal a malignant and advanced tumor, primarily in the parotid gland.
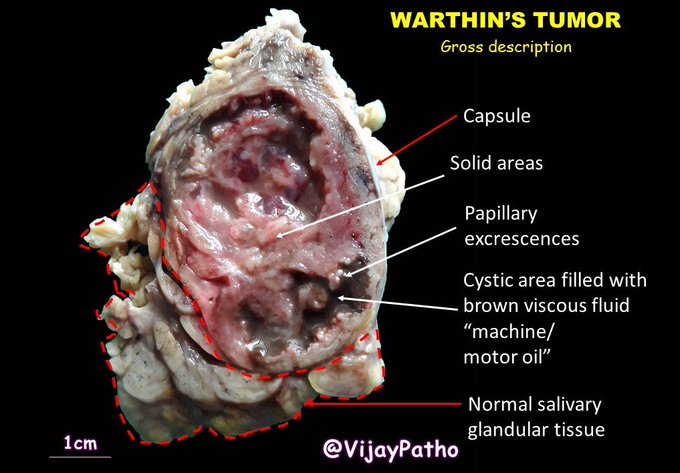
Gross Pathology
- Encapsulated
- Smooth/lobulated surface
- Soft, fluctuant, compressible
- Cystic spaces of variable size, with viscous fluid, shaggy epithelium
- The size of a Warthin tumor can vary from a few millimeters to several centimeters •Solid areas with white nodules representing lymphoid follicles
Image Credit: https://x.com/VijayPatho/status/1019578913863823360
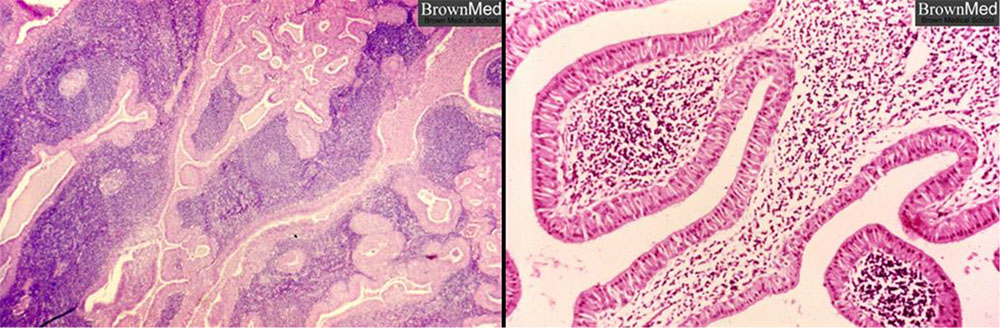
Histology
- Thin capsules usually sharply demarcate tumor from surrounding parenchyma.
- Cystic spaces are lined by a papillary proliferation of bilayered, oncocytic epithelium whose supporting stroma is composed largely of lymphoid tissue
- Dense lymphoid stroma with double layer of epithelial cells resting on the stroma.
- The cystic spaces are present which are narrowed by polypoid projections.
- Basal cell layer is not continuous and is interrupted in places .
- The oncocytic columnar cells palisade on the surface.
- There is no myoepithelial component present in tumor.
- Occasional features include cilia, squamous metaplasia with necrosis, mast cells, dendritic cells and sebaceous cells.
Diagnosis
- X-rays of the salivary gland (called a sialogram) to look for a tumor
- Ultrasound, CT scan or MRI to confirm that there is a growth, and to see if it has spread to lymph nodes in the neck
- Salivary gland biopsy or fine needle aspiration to determine whether the tumor is benign or malignant
- Sialendoscopy, a minimally invasive outpatient procedure, used to identify small tumors that may otherwise go unnoticed and progress to later-stage cancer
- Positron emission tomography (PET) scans may be of value in assessing malignant tumors, with attention to metastatic adenopathy and distant metastases
Treatment
- The treatment involves a surgical procedure to remove the neoplastic lesion.
- This procedure is relatively easy due to the favorable, superficial location of the tumor.
- The exact method of tumor removal depends on its precise location. In many cases, a so-called Parotidectomy is performed, which involves the surgical removal of a part or all of the parotid gland.
- This procedure minimizes the risk of relapse.
Prognosis
- Due to the benign nature of Warthin's tumor, the overall prognosis is good
- Possible complications result from the risk of damage to the facial nerve during surgery (this nerve courses through the parotid).
Related posts
April 10, 2025
April 9, 2025
April 4, 2025
