- NEED HELP? CALL US NOW
- +919995411505
- [email protected]
NEPHROTIC SYNDROME
Definition
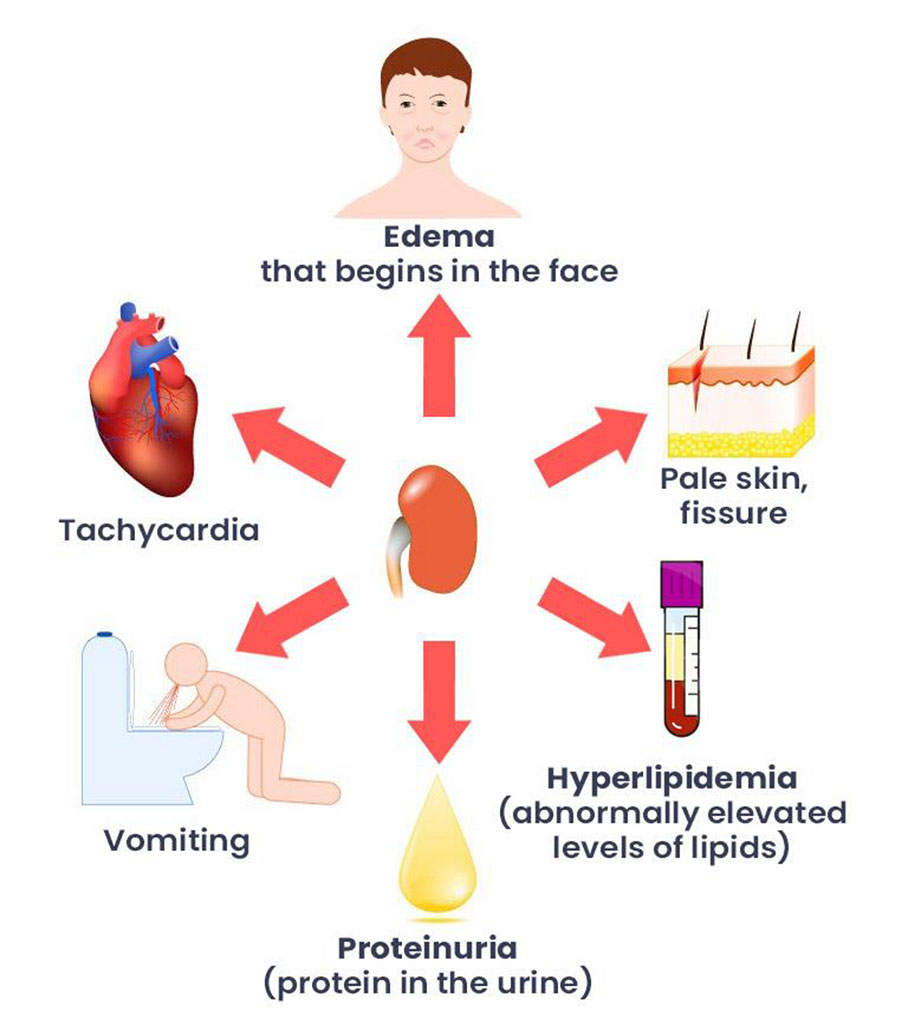
Nephrotic syndrome is a clinical complex characterized by a number of renal and extrarenal features, most prominent of which are
- Proteinuria (in practice > 3.0 to 3.5gm/24hrs),
- Hypoalbuminemia,
- Edema,
- Hypertension
- Hyperlipidemia,
- Lipiduria and
- Hypercoagulabilty.
Etiology
| Primary or idiopathic , being a disease specific to the kidneys |
| Secondary or genetic, being a renal manifestation of a systemic general illness |
| Congenital very rare |
| Primary causes include | Secondary causes include |
|
|
Incidence
- 2 – 7 cases per 100,000 children per year
- Higher in underdeveloped countries (South east Asia )
- Occurs at all ages but is most prevalent in children between the ages 1.5-6 years.
- It affects more boys than girls, 2:1 ratio
*Nephrotic syndrome is 15 times more common in children than in adults.
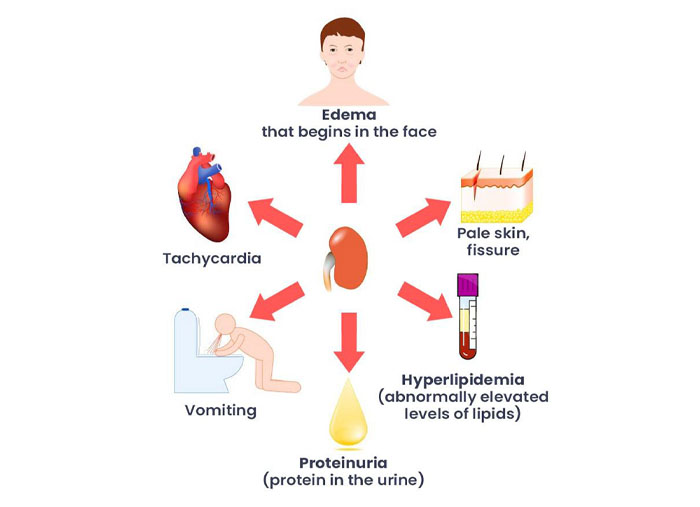
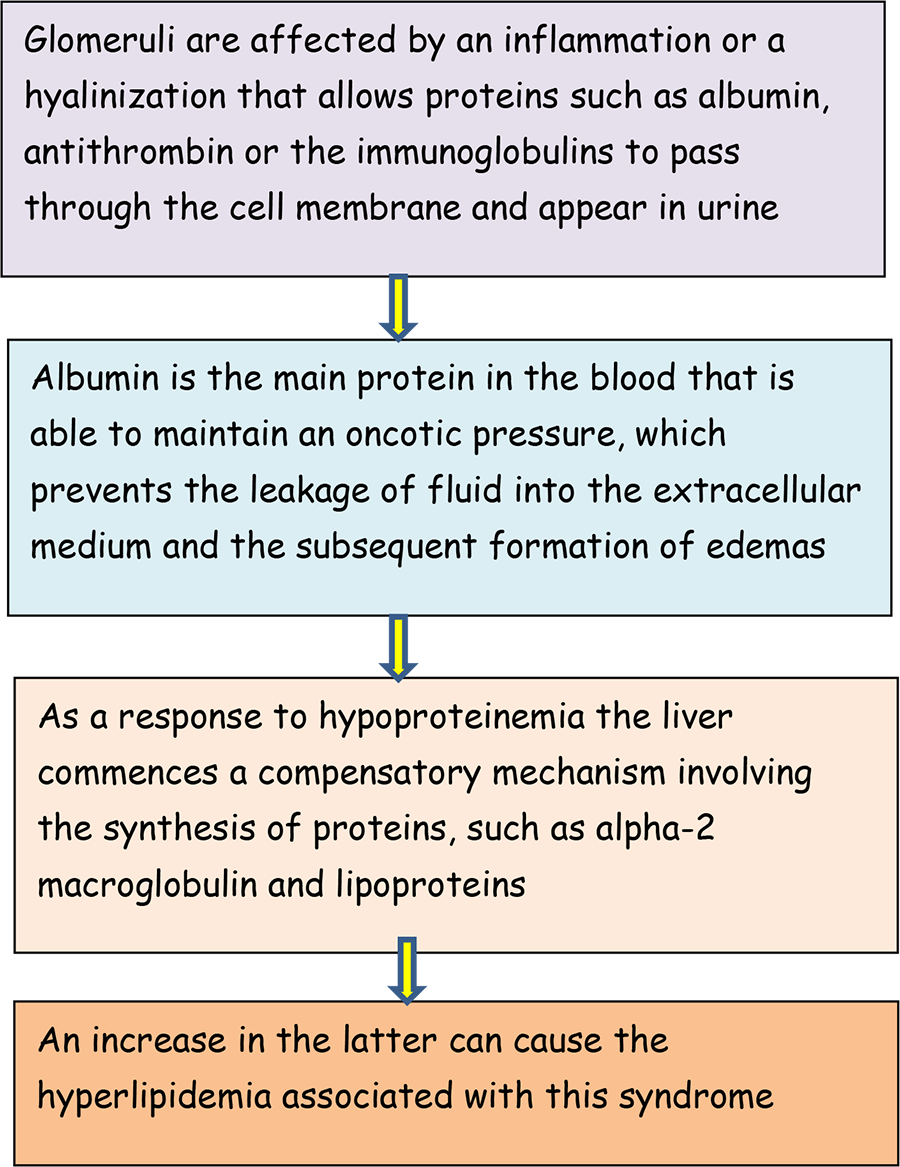
Pathophysiology
Symptoms
- Puffy eyelids and swelling in the legs, ankles, feet, lower abdomen, or other parts of your body
- Foamy urine
- Weight gain due to retaining too much fluid
- Tiredness
- Vomiting
- Loss of appetite
Investigation
1-Urine analysis:-
- Proteinuria: 3-4 + selective.
- 24 urine collection for protein >40mg/m2/hr for children
- Volume: oliguria (during stage of edema formation)
- Microscopically:- microscopic hematuria 20%, large number of hyaline cast
2-Blood:
- Serum protein: decrease >5.5gm/dl , Albumin levels are low (<2.5gm/dl).
- Serum cholesterol and triglycerides: Cholesterol >5.7mmol/L (220mg/dl).
- ESR↑>100mm/hr during activity phase
3. Serum complemen: Vary with clinical type.
4. Renal function
5. Biopsy in case of
- Secondary N.S,
- Frequent relapsing N.S,
- Steroid resistant N.S,
- Haematuria,
- Hypertension,
- Low GFR
Treatment
Depend on the cause of your nephrotic syndrome.
Any other condition is to blame, that will be the first thing to treat. Lowering your cholesterol and blood pressure as well as reducing edema may be key
goals.
Medicines you might take include:
- Blood-pressure medications called ACE inhibitors and ARBs, which curb the pressure in your glomeruli and lower the amount of protein in your
urine - Diuretics, or water pills, to reduce swelling
- Cholesterol-lowering drugs
- Blood thinners, or anticoagulants, to make blood clots less likely
- Medications that turn down your immune system, such as corticosteroids
Complications
- Thromboembolic disorders.
- Infections: The increased susceptibility of people with nephrotic syndrome to infections can be a result of the leakage of immunoglobulins from the blood, the loss of proteins in general, and the presence of oedematous fluid (which acts as a breeding ground for infections).
- Spontaneous bacterial peritonitis can develop where there is ascites present. This is a frequent development in children but very rarely found in adults.
- Acute kidney failure due to hypovolemia
- Pulmonary edema: the loss of proteins from blood plasma and the consequent fall in oncotic pressure causes an abnormal accumulation of liquid in the lungs causing hypoxia and dyspnoea.
- Hypothyroidism: deficiency of the thyroglobulin transport protein thyroxin (a glycoprotein that is rich in iodine and is found in the thyroid gland) due to decreased thyroid-binding globulin.
- Vitamin D deficiency
- Hypocalcaemia: lack of 25-hydroxycholecalciferol (the way that vitamin D is stored in the body). As vitamin D regulates the amount of calcium present in the blood, a decrease in its concentration will lead to a decrease in blood calcium levels. It may be significant enough to cause tetany. Hypocalcaemia may be relative; calcium levels should be adjusted based on the albumin level and ionized calcium levels should be checked.
- Microcytic hypochromic anaemia: iron deficiency caused by the loss of ferritin (compound used to store iron in the body). It is iron-therapy resistant.
- Protein malnutrition: this occurs when the amount of protein that is lost in the urine is greater than that ingested, this leads to a negative nitrogen balance
- Growth retardation: This can occur in cases of relapse or resistance to therapy. Causes of growth retardation are protein deficiency from the loss of protein in urine, anorexia (reduced protein intake), and steroid therapy (catabolism).